By Eric Andrew Kristof, RN, CAHIMS | Healthcare IT Professional | HIMSS Arkansas Chapter Member
About This Series: The HIMSS Word of the Day is a running blog series drawing from the HIMSS Dictionary of Health Information and Technology Terms, Acronyms, and Organizations, 6th Edition (2025) — the authoritative reference for healthcare IT professionals and the primary study resource for CAHIMS and CPHIMS certification. Each post paraphrases the term in plain language, grounds it in real-world healthcare IT context, and adds a bedside nursing perspective you won’t find in a textbook.
📖 The Term: Accountable Care Organization (ACO)
Source: HIMSS Dictionary of Health Information and Technology Terms, Acronyms, and Organizations, 6th Edition (2025)
🔍 Plain-Language Definition
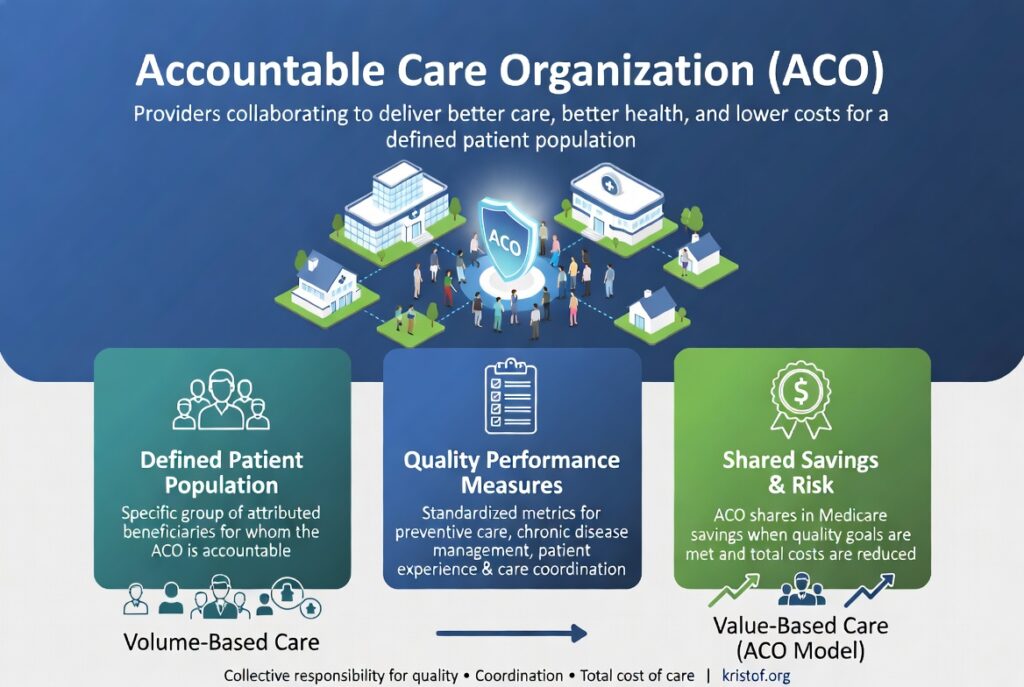
An Accountable Care Organization (ACO) is a voluntary network of physicians, hospitals, and other healthcare providers who come together to take collective responsibility for the quality, coordination, and total cost of care for a defined patient population.
The model rests on a simple bargain: deliver high-quality, coordinated care that prevents medical errors and eliminates wasteful duplication — particularly for chronically ill patients — and the organization shares in the savings it generates for Medicare or another payer. ACOs are the most prominent operational expression of the broader shift from volume-based to value-based reimbursement.
Three operational elements define a functioning ACO:
| Element | Description |
|---|---|
| Defined Patient Population | A specific group of attributed beneficiaries for whom the ACO is accountable, typically assigned via primary care relationships |
| Quality Performance Measures | A standardized set of metrics — preventive care, chronic disease management, patient experience, and care coordination — against which the ACO is evaluated |
| Shared Savings / Risk Arrangement | A financial contract with the payer (most commonly CMS) that lets the ACO share in cost savings, and in some models, share in losses |
⚠️ Exam Alert: Don’t confuse the ACO (the organization) with the Medicare Shared Savings Program (one of several federal programs an ACO may participate in), the Patient-Centered Medical Home (a primary care delivery model that may be a building block of an ACO), or Pay-for-Performance (the reimbursement mechanism underlying ACO financial incentives). CAHIMS questions routinely swap these terms.
🌐 Why It Matters: Real-World Healthcare IT Context
ACOs are not just policy abstractions — they are health IT mandates in disguise.
No organization can be “accountable” for a population it cannot see. The technical and informatics infrastructure required to operate a successful ACO is enormous: longitudinal patient records spanning multiple care settings, real-time risk stratification, gap-in-care analytics, care coordination workflows, and quality measure reporting straight from EHR data.
The dominant federal ACO program is the Medicare Shared Savings Program (MSSP), administered by CMS since 2012. Other prominent models have included the Pioneer ACO, the Next Generation ACO, Direct Contracting, and the current ACO REACH (Realizing Equity, Access, and Community Health) model. Each varies in risk arrangement, beneficiary attribution methodology, and quality measure set.
Without robust health IT, ACOs cannot:
- Identify which patients are attributed to them at any given moment
- Stratify their population by clinical, social, and financial risk
- Coordinate care across primary care, specialty care, behavioral health, and post-acute facilities
- Track quality measure performance against benchmark thresholds
- Calculate shared savings and submit accurate cost reports
With mature ACO-grade health IT:
- Population health dashboards surface care gaps proactively
- Risk-stratification algorithms target intensive care management to the highest-need patients
- Care coordinators receive automated alerts on ED visits and hospitalizations
- Annual wellness visit completion and preventive screening rates improve measurably
- Quality measure submissions are automated, auditable, and tied to clinical workflow
For anyone building, configuring, or analyzing health IT systems in an organization with ACO contracts, the ACO’s quality and financial requirements are often the operational North Star.
🏥 The Nurse’s Perspective: Clinical, Bedside, & Workflow
The ACO model lives in nursing workflow whether the bedside team knows the acronym or not.
At the Bedside
Nurses see the ACO model show up as discharge workflow. Care coordinators arrive at the bedside for high-risk patients, transition-of-care documents must be complete before the patient leaves, and readmission risk scores appear in the EHR. None of that is decoration — readmissions and care gaps are exactly what ACO quality metrics measure, and the documentation nurses enter feeds those metrics directly.
Pre-discharge teach-back, medication reconciliation, and outpatient follow-up scheduling — long considered “soft” nursing work — are revealed as hard financial determinants in the ACO model. A botched discharge that results in a 30-day readmission costs the ACO real money, and the bedside nurse is the last line of defense against that outcome.
In Clinical Workflow
Nursing workflows in ACO-affiliated organizations look fundamentally different from fee-for-service workflows. Annual wellness visit checklists, depression screenings, falls risk assessments, and tobacco cessation counseling become structured EHR fields with required completion. Care plans extend beyond the four walls of the hospital to include home health, skilled nursing facility transitions, and ambulatory follow-up.
Population health nurses — a relatively new role in many organizations — sit between the EHR’s risk-stratification dashboards and the bedside. They reach out to attributed patients before crises, coordinate transitions, and close care gaps. That role is clinical informatics in action.
In EHR Implementation (Go-Live Perspective)
During Epic Go-Lives in ACO-affiliated organizations, build decisions are explicitly informed by ACO quality measure requirements. Healthy Planet (Epic’s population health module), care management workflows, and registries for diabetic, hypertensive, and heart failure populations are configured around CMS quality measure specifications.
When build teams ask whether a given prompt should be a hard stop or a soft alert, the answer often traces back to an ACO measure. When end-user training emphasizes a specific documentation field, that field is often a quality measure data element. ACOs make EHR configuration choices visible and consequential.
🎓 CAHIMS / CPHIMS & HIMSS Perspective
CAHIMS Exam Domain Mapping
ACOs appear in CAHIMS exam content across multiple domains:
| CAHIMS Domain | How ACO Appears |
|---|---|
| Healthcare & Technology Environments | Federal programs (MSSP, ACO REACH); CMS quality measure frameworks; value-based care policy landscape |
| Clinical Informatics | Population health analytics; risk stratification; care coordination workflows; clinical decision support for chronic disease management |
| Healthcare Information & Systems Management | Health information exchange across ACO partners; data warehousing for quality reporting; master patient index challenges in beneficiary attribution |
| Management & Leadership | Organizational structure of ACO partnerships; physician engagement; change management for value-based care transition |
Key Terms to Know Alongside ACO
- Medicare Shared Savings Program (MSSP) — the largest CMS ACO program; the operational vehicle most “ACOs” actually participate in
- Patient-Centered Medical Home (PCMH) — a primary care delivery model emphasizing care coordination; often a foundational building block of an ACO
- Pay-for-Performance (P4P) — the reimbursement mechanism that ties payment to quality and cost outcomes; the financial underpinning of ACO contracts
- Value-Based Care — the broader policy paradigm shifting reimbursement from volume to value, of which the ACO model is a leading expression
- Capitation — a payment model in which providers receive a fixed amount per patient regardless of services delivered; related to, but distinct from, ACO shared savings
- Population Health Management — the systematic effort to improve health outcomes for a defined group; the operational discipline ACOs depend on
HIMSS Organizational Position
HIMSS actively supports the value-based care transition through its Population Health and Care Coordination programming, ongoing policy engagement with CMS and ONC, and annual Global Health Conference content. HIMSS members can access ACO-focused webinars, case studies, and implementation toolkits through the member portal.
🔗 Explore Further: External References
- CMS — Medicare Shared Savings Program https://www.cms.gov/medicare/medicare-fee-for-service-payment/sharedsavingsprogram
- CMS Innovation Center — ACO REACH Model https://www.cms.gov/priorities/innovation/innovation-models/aco-reach
- HealthIT.gov — Value-Based Care and Health IT https://www.healthit.gov/topic/value-based-care
- HIMSS — Population Health Resource Hub https://www.himss.org/resources/population-health
- National Association of ACOs (NAACOS) https://www.naacos.com
- MedPAC — Annual Reports on Medicare Payment Policy https://www.medpac.gov
Term source: HIMSS Dictionary of Health Information and Technology Terms, Acronyms, and Organizations, 6th Edition (2025). All definitions in this series are paraphrased for editorial purposes. Readers are encouraged to consult the primary source for exact language.
Eric Andrew Kristof, RN, CAHIMS is a Healthcare IT professional and HIMSS Arkansas Chapter member based in Hot Springs Village, AR, with hands-on Epic Go-Live experience and a diverse healthcare and IT background. He writes at kristof.org at the intersection of clinical care and healthcare technology.
Leave a Reply